





Understanding GLP-1: How Ozempic & Co. work, who really needs them, and why muscle mass is crucial for safe weight loss.


GLP-1 medications (Ozempic, Wegovy, Mounjaro) have officially crossed the line from targeted medical treatment to global cultural obsession. Between the viral hashtags and the promises of a miracle cure, the 2026 data reveals a much more complex biological reality. The real question is not whether these drugs work. They do. The question is whether you understand what they are actually doing to your body. By André Pedro
THE BIOLOGY: THE OFFICE SHREDDER IN YOUR GUT
Your body was built to survive famine, not to resist a Coop Pronto at 8pm.
Human biology is evolutionarily programmed for scarcity. Whenever you eat, your gut releases a hormone called GLP-1, a messenger that signals the brain to register fullness and tells the pancreas to manage blood sugar. Simple enough.
The problem is that natural GLP-1 is extremely short-lived. An enzyme called DPP-4 acts as a hyper-efficient biological shredder, destroying the fullness signal in approximately 90 seconds (Nauck & Quast, 2021). Evolution designed this to keep you eating in environments where food was scarce. Useful for a caveman; less helpful when you are walking past a fresh Butterzopf display at the train station.
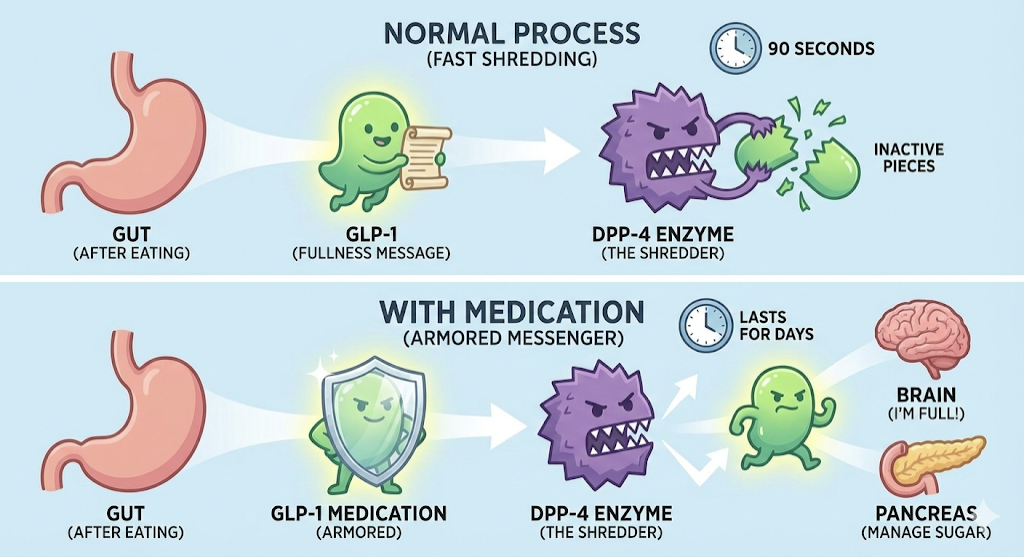
Graph 1: the mechanism of GLP-1 and the «shredder» enzyme DPP-4. AI-generated (2026).
Modern GLP-1 medications are shredder-proof. Engineered to resist the DPP-4 enzyme, they circulate in the system for an entire week, creating a sustained signal of satiety and effectively lowering the volume on the constant food noise that defines modern life.
WHO ARE THESE MEDICATIONS ACTUALLY FOR?
GLP-1 agonists are not lifestyle drugs. They are metabolic medicine with specific clinical criteria.
Current clinical guidelines indicate these medications for adults with a BMI of 30 or above, or a BMI of 27 or above in the presence of at least one weight-related comorbidity: type 2 diabetes, hypertension, or cardiovascular disease. This distinction matters, and it sets the stage for everything that follows.
BEYOND THE SCALE: WHAT THESE DRUGS DO TO YOUR ORGANS
The cardiovascular and renal data is where this science becomes genuinely impressive.
The SELECT trial (NEJM, 2023), involving over 17,600 participants, recorded a 20% reduction in major adverse cardiovascular events. Importantly, this population was specifically adults with overweight or obesity, established cardiovascular disease, and no type 2 diabetes; meaning the cardiac benefit appears to operate independently of glucose management, likely through a reduction in systemic arterial inflammation.
On kidney health, the FLOW trial (Perkovic et al., 2024) proved so effective at preserving kidney function in patients with type 2 diabetes that the study was halted early. Independent committees determined it would be unethical to withhold the treatment from the placebo group given the undeniable evidence.
On bone density, a 2025 meta-analysis (Alalwani et al.) found that GLP-1 agonists may help attenuate the bone loss typically associated with rapid weight reduction, a clinically relevant finding, though the evidence remains mixed across different populations and warrants cautious interpretation.
THE MENTAL SHIFT: SILENCING FOOD NOISE
For many people, hunger is not a physical sensation: it is a constant, exhausting mental preoccupation.
GLP-1 acts on the hypothalamus, the brain’s metabolic command centre, stabilising satiety signals and reducing the impulsive drive to eat. This is not a matter of willpower. It is the biological recalibration of a signal that was previously running at full volume, all the time. For many patients, this is the first time in their lives that food is simply not the main character.
THE AESTHETIC HIJACKING: A GROWING PROBLEM
Using a systemic metabolic drug for minor cosmetic tweaks is biologically disproportionate.
In Brazil, and increasingly here in Switzerland, a growing number of people with healthy BMIs are using these medications to lose small amounts of weight for aesthetic purposes. This is a problem.
When GLP-1 agonists are used without significant adiposity, the body enters a state of metabolic pressure. Without sufficient fat reserves to draw from, the system will increasingly break down muscle tissue to meet its energy demands. The result is accelerated metabolic ageing and a loss of structural integrity, regardless of what the scale says.
THE MUSCLE PROBLEM: THE HUMAN GUMMY BEAR EFFECT
Losing weight and losing fat are not the same thing. This distinction can define the long-term outcome.
A 2025 systematic review (Berg et al.) indicates that lean mass loss can account for nearly 40% of total weight lost when no protective strategy is in place. For vegetarians, the risk is compounded; without adequate protein intake, and specifically the amino acid leucine which triggers muscle protein synthesis, the body will actively scavenge its own muscle tissue to maintain vital functions.
Rapid weight loss without a muscle-first strategy produces what can only be described as medicated frailty: soft, structurally weak, and with a metabolism slower than a Sunday morning in Appenzell.
MYTHS AND THE FINE PRINT
Most of the fear around GLP-1 medications is either exaggerated or factually wrong.
“Ozempic Face” is a toxic side effect. It is not. Facial fat loss is a natural consequence of rapid overall weight reduction. When the fat pads that provide volume and structural support disappear quickly, the skin can appear loose or aged. This is a speed-of-loss issue, not a drug-specific reaction.
The drugs cause permanent stomach paralysis. GLP-1 medications work by slowing gastric emptying. Severe gastroparesis is reported in a very small fraction of cases (under 1%), and most gastrointestinal symptoms are dose-dependent and temporary. Trying to eat a heavy cheese fondue while your digestion is already slowed down is not a side effect; it is a predictable consequence of ignoring how the drug works.
Weight regain is inevitable. Regain is common when the medication is treated as a magic wand rather than a window of opportunity. Data from West et al. (BMJ, 2026) suggests regain after cessation averages approximately 0.8 kg per month in those who do not implement sustainable lifestyle changes. The drug creates quiet time. What you build during that time determines the outcome.
The thyroid cancer risk is high. Large-scale human trials involving tens of thousands of participants have not shown a statistically significant increase in thyroid cancer. Initial concerns came from rodent studies, and rodent thyroid biology differs substantially from humans.
THE EXIT STRATEGY: BUILD THE ROAD WHILE YOU HAVE THE BRIDGE
The medication is a temporary signal. The habits are permanent.
The data from 2026 confirms that GLP-1 is not a genetic fix; it is a bridge. The goal during treatment is to build the road on the other side: resistance training to preserve and build lean mass, nutritional density to support recovery and organ function, and behavioural anchors that do not depend on the drug to hold.
Two practical points that are consistently underestimated:
Satiety recognition: digestion is slowed, meaning the fullness signal arrives late. Eating past the first sign of satisfaction is not just a mistake; it is a reliable invitation for reflux and nausea several hours later.
Hydration: GLP-1 can reduce the thirst drive. A significant portion of the fatigue and brain fog commonly attributed to the medication is, in reality, straightforward dehydration.
THE VERDICT
GLP-1 is arguably the most significant advance in metabolic medicine in decades. It is also being systematically misused.
For the right patient – with clinical indication, adequate protein intake, and a structured resistance training programme – the data is compelling. The drug silences the noise, protects the organs, and creates a window for real metabolic change.
Without the muscle-first strategy, that window closes, and what remains is a lighter body with a slower metabolism and less structural integrity than before. The science supports the tool. Whether the tool is used wisely depends entirely on what surrounds it.
SCIENTIFIC REFERENCES
- Alalwani, Y. J., et al. (2025). Differential effects of GLP-1 receptor agonists on bone mineral density: A patient-stratified network meta-analysis. BMC Musculoskeletal Disorders.
- Berg, S., Stickle, H., Rose, S. J., & Nemec, E. C. (2025). Discontinuing glucagon-like peptide-1 receptor agonists and body habitus: A systematic review and meta-analysis. Obesity Reviews, 26(8), e13929.
- Lincoff, A. M., et al. (2023). Semaglutide and cardiovascular outcomes in obesity without diabetes (SELECT Trial). New England Journal of Medicine, 389(24), 2221–2232.
- Nauck, M. A., Quast, D. R., Wefers, J., & Meier, J. J. (2021). GLP-1 receptor agonists in the treatment of type 2 diabetes: state-of-the-art. Molecular Metabolism, 46, 101102.
- Perkovic, V., et al. (2024). Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes (FLOW Trial). New England Journal of Medicine.
- West, S., et al. (2026). Weight regain after cessation of medication for weight management: Systematic review and meta-analysis. The BMJ.
- Wilding, J. P. H., et al. (2021). Once-weekly semaglutide in adults with overweight or obesity (STEP 1 Trial). New England Journal of Medicine, 384(11), 989–1002.



Challenge of the Month

What Clients Say





What You Get


